If a casualty is unresponsive, medical alert tags, bracelets or cards may provide information about pre-existing medical conditions. Prescribed medical equipment may also be an indicator of a pre-existing medical condition.
A structured assessment of the casualty should be carried out by a competent person, with the necessary equipment and using the following approach:
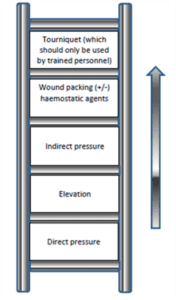
- <C> Control of catastrophic external compressible bleeding
- The use of tourniquets, by trained personnel, forms part of the Faculty of Pre-Hospital Care (FPHC) position statement.
- If there is a concern that a major bleed may occur on the casualty’s release, tourniquet(s) may be applied loose, prior to extrication. These can then be quickly tightened if required – this action should only be undertaken by trained personnel.
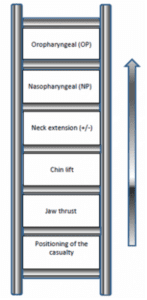
- Airway
- A simple ‘airway ladder’ approach to airway care should be promoted
- Assessment and monitoring of the airway should be continuous
- Suction should be available to clear the airway